What are some common symptoms?
Symptoms associated with bacterial meningitis come about rapidly over a period of 3-7 days after being exposed. In newborns and infants, common symptoms like fever, headaches, and stiff neck are difficult to identify. Infants that are infected are difficult to comfort and could produce louder than normal crying when picked up. In addition to these signs, infants may demonstrate signs that include:[20][21]
- High fever
- Constant crying
- Excessive sleepiness or irritability
- Inactivity or sluggishness
- Poor feeding
- A bulge in the soft spot on top of the head (fontanel)
- Stiffness in the body and neck
- Seizures
- High fever
- Severe headache
- Stiff neck
- Vomiting or nausea with headache
- Confusion or difficulty concentrating and may seem like the inability to maintain eye contact for children
- Seizures
- Sleepiness or difficulty waking up
- Sensitivity to light
- Lack of appetite
- Skin rash in some cases like meningococcal meningitis
What is the epidemiology behind bacterial meningitis?
Bacterial meningitis is responsible for infecting 8000 individuals and causing 2000 deaths annually. In the United States there are about 0.6 to 4 cases for every 100,000 people. In developing parts (ex. Africa & India) of the world, Meningococcal meningitis is known to be an endemic. In the sub-Suharan region and among religious travelers, Saudi Arabia cyclical epidemics of bacterial meningitis are known to occur. Furthermore, frequent epidemics take place in various regions of Africa. The largest outbreak of meningococcal meningitis took place across West Africa in 1996. In this epidemic, about 250,000 individual were infected which caused about 25,000 deaths. In newborns, there are about 0.25 to 1 cases for every 1000 live births which can be broken down to 0.15 cases per 1000 full-term births and 2.5 cases per 1000 premature births. [25]
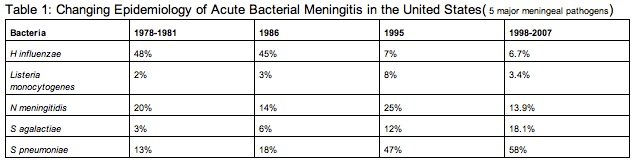
The incidence of neonatal bacterial meningitis is 0.25-1 case per 1000 live births. In addition, the incidence is 0.15 case per 1000 full-term births and 2.5 cases per 1000 premature births. On average 30% of newborn sepsis can be linked to bacterial meningitis. Looking at Table 1 [25] below, it is evident that infections caused by H influenzae type B and N meningitidis once were responsible for over 80% of cases, but have now been significantly reduced in the past decades because of several developments.
Today, infection in children ages 1 to 23 months of age is caused by N meningitidisis for about 4 cases per 100,000 children and by S pneumoniae for about 6.5 cases per 100,000 children. As the decline of bacterial meningitis continues, this disease has become predominant in adults. The median age for a person infected was 15 months in 1986 and dramatically increase to 25 years in 1998.
Moreover, a rise among HIV infections has resulted in a rise of meningitis caused by encapsulated bacteria, especially S pneumoniae. Over the years bacterial meningitis infections have been on the decline largely because of current use of H influenzae type B (HIB) vaccinations which lowered the occurrence of HIB meningitis by over 90%. From 1993 to 2003, a ten year period, bacterial meningitis dropped from 1.9 to 1.5 cases per 100,000 people. [25]
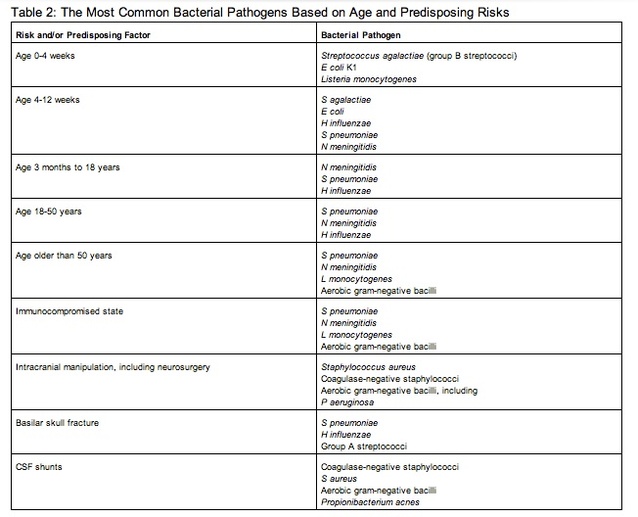
The use of vaccines that provide protection against S pneumoniae has allowed for a decrease in pneumococcal meningitis in children. In addition, frequent screening of pregnant women for the presence of S agalactiae related meningitis has caused a reduction of meningitis. These measures along with the HIB vaccine have caused the incidence of meningitis to drop by 31%, according to a 1998-2007 survey. Although significant advancements have been made to prevent and treat bacterial meningitis to a point that the mean age for those infected is about 25, individuals younger than 5 years and over 60 years are at greatest risk of bacterial meningitis, excluding meningococcal meningitis. For infants, climax incidence is at 3 to 8 months of age. Today, the average yearly incidence in adults is about 3.8 cases per 100,000. Out of the patients that have become infected with bacterial meningitis, 61% were reported to have had no current disease that could have promoted meningitis. As new treatments and methods of preventing bacterial meningitis are developed, the epidemiology behind bacterial meningitis continues to change. Table 2 [25] below lists the common bacteria that infect an individual depending on their age.[25]
How is it diagnosed?
If an individual is suspected of having bacterial meningitis, there are specific methods for diagnosing an infection. Test used today to identify a positive infection of bacterial meningitis include: [21]
- Blood cultures: In this test blood is obtained from a vein and is handed off to a lab. In the lab the blood is placed in a dish to obbserve if bacteria grow in the blood. Furthermore, collected blood can be placed on a slide and stained in order to check for the presence of bacteria.[21]
- Imaging: Imaging modalities like X-rays and computerized tomography (CT) scans of head, chest or sinuses can be utilized to identify the presence of swelling or inflammation. Thus,doctors can utilize these imaging modalities to identify the presence of infections due to meningitis.[21]
- Spinal tap (lumbar puncture). This method provides an absolute diagnosis of bacterial meningitis. This diagnosis method involves the analysis of an individuals cerebrospinal fluid (CSF). The CSF is obtained via a spinal tap. CSF that belongs to an infected individual has low glucose levels, and an elevated count of white blood cells and proteins. In addition, this method can allow for the exact identification of the bacteria at fault.[21]
How is it treated?
Antibiotic Therapy
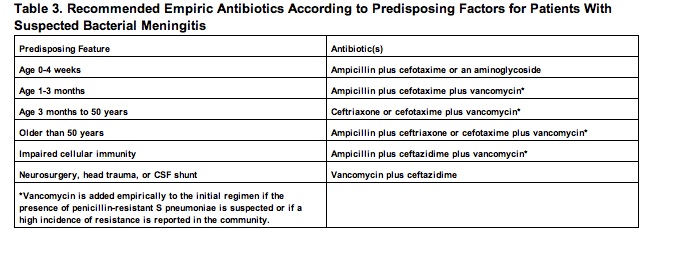
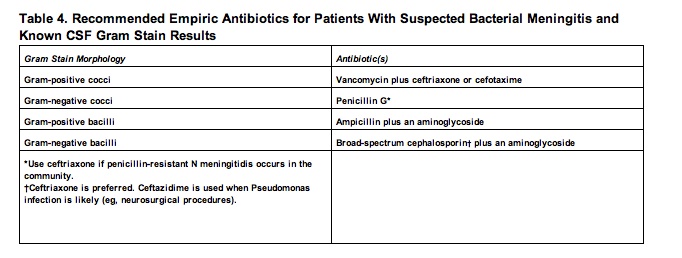
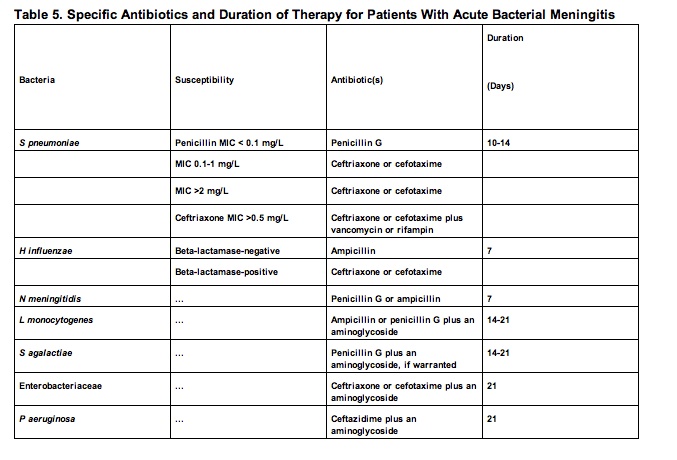
In order for an infected patient to have a better recovery, the initiation of empiric antibacterial therapy is essential prior to identifying the exact pathogen. After proper identification through a CSF analysis has been made, ideal antibiotic treatment can be administered. In The Sanford Guide to Antimicrobial Therapy, a list of recommended empiric antibiotics therapies is listed according to age in Table 3 [18] below. In Table 4 [18] empiric antibiotics therapies based on the CSF Gram stain results is listed. In Table 5 [18] antibiotic therapies are listed for when the bacterial pathogen is known. [18]
Antibiotic Therapy
In order for an infected patient to have a better recovery, the initiation of empiric antibacterial therapy is essential prior to identifying the exact pathogen. After proper identification through a CSF analysis has been made, ideal antibiotic treatment can be administered. In The Sanford Guide to Antimicrobial Therapy, a list of recommended empiric antibiotics therapies is listed according to age in Table 3 [18] below. In Table 4 [18] empiric antibiotics therapies based on the CSF Gram stain results is listed. In Table 5 [18] antibiotic therapies are listed for when the bacterial pathogen is known. [18]
Steroid therapy
Today, the use of steroids have proven to reduce inflammation resulting from the human defense system and improving the overall recovery with certain bacterial meningitis such as H influenzae, tuberculous, and pneumococcal meningitis. One of the most widely used steroids is dexamethasone. This steroid has resulted in lowered amounts of hearing loss and neurological sequelae in children and infants that have HIB bacterial meningitis. [18]
Today, the use of steroids have proven to reduce inflammation resulting from the human defense system and improving the overall recovery with certain bacterial meningitis such as H influenzae, tuberculous, and pneumococcal meningitis. One of the most widely used steroids is dexamethasone. This steroid has resulted in lowered amounts of hearing loss and neurological sequelae in children and infants that have HIB bacterial meningitis. [18]
